 Book an Appointment
Book an Appointment




Acoustic Neuroma (also known as Schwannoma or Vestibular Schwannoma), frequently misdiagnosed as brain tumor caused by the growth of the schwann cells along the auditory neuron. Auditory neuroma accounts for 8% of all intracranial brain tumors. In terms of regional division, Cerebellopontine angle (CPA) tumors is the most common brain tumor which accounts for approximately 80 to 90% of all Cerebellopontine angle (CPA) tumors.
The auditory and vestibular nerve of the human body are connected from the inner ear to the brain stem. Acoustic neuroma is a slow-growing benign tumor, with an average growth of 1 to 2 mm per year. Generally speaking, 90% of patients’ tumors are mostly located on the left or right side. 10% of patients have tumors on the left and right sides appearing at the same time or at different times in sequence. Speaking of acoustic neuroma, people will often overestimate the severity once it grows in the brain, but it is not. The onset of acoustic neuroma is mild and slow with the initial symptom of tinnitus, however, it is still easily to be misdiagnosed.
Enlarged tumor can cause paralysis and weakness of facial muscles
It is mainly caused by the compression of the tumor on the 5th, 7th and 8th cranial nerves.
1) Auditory nerve and vestibular nerve: The patients most often suffers from hearing loss and tinnitus (95%), dizziness is rare (61%).
2) Trigeminal nerve: 17% of patients have facial numbness, facial sensitivity to sensory stimulation, or pain.
3) Facial nerve: only about 6% of patients will have facial muscle weakness or having abnormal tastes in their mouth.
4) Others: When the tumor compresses the cranial nerves 9th, 10th, and 11th, the patient will have difficulty swallowing and problems with pronunciation.
If the tumor is too large and compresses to the cerebellum or brainstem, there will be muscle weakness,unstable gait, body imbalance. If the situation is more serious, there will be a risk of hydrocephalus and even death.
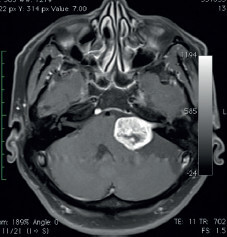
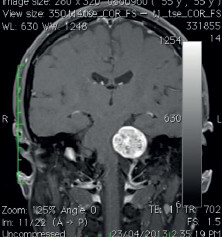
MRI Imaging Diagnosis
MRI imaging examination is helpful for the clear diagnosis and identification of tumors in the cerebellopontine angle area, such as meningioma, epidermoid cyst, trigeminal schwannoma, etc.
It can be seen that the auditory neuroma grows from the inner auditory canal to the inside,
Like the tail of a tadpole:
Tumor pressure on the cerebellum and brain stem:
Considering minimally invasive microscopic surgery for tumors that are large or nerve compression
Neurosurgeons will consider and evaluate various aspects for appropriate treatment. If the tumor is small and asymptomatic, the patient can be followed up and checked regularly with a conservative treatment plan. If the tumor is large or compressed nerves, and the patient has serious symptoms, neurosurgeons will consider using minimally invasive surgical removal with a microscope.
Minimally invasive microscope surgery to protect the auditory and facial nerve
Generally speaking, minimally invasive microscopic surgery is the method for radical treatment of acoustic neuroma, but due to the proximity between the tumor, the nerve, and the brainstem, there are certain risks during the operation, especially hearing loss due to auditory nerve damage, or facial muscles nerve damage is more likely to cause facial paralysis. However, experienced neurosurgeons will perform skilled and delicate operations under the microscope, using continuous Intraoperative Neural Monitoring System IOM,greatly improves the functional preservation of auditory nerve and facial muscle nerve. Experienced neurosurgeons have a total tumor resection rate of 97 to 100%, a functional preservation rate of facial muscles and nerves of 51 to 98.2%, a hearing preservation rate of 19 to 40%, and a tumor recurrence rate of 5 to 10%.

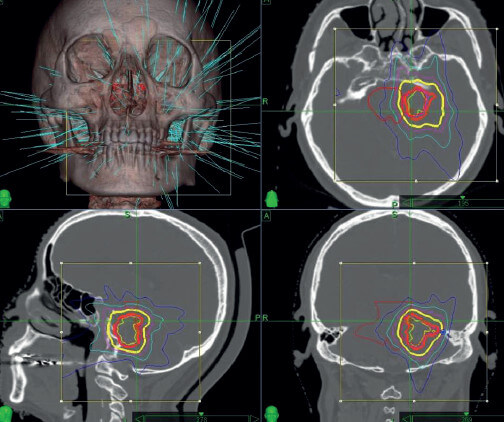
Cyberknife Procedure
Cyberknife is suitable for tumors below 3 cm or residual tumors after surgery and elderly patients. Cyberknife has relatively low risk, fast recovery and short treatment time, usually 3 to 7 days. The therapeutic effect is related to the radiation dose, but this method is not recommended for the tumors with cystic changes and obvious brain stem compression. The goal of its treatment is to kill tumor cells or control the growth of tumor cells through high-energy rays. In the short term after radiotherapy, the tumor may be swollen and enlarged. Therefore, dehydration and lowering of intracranial pressure may be needed in the short term. The results of medical literature analysis show that the tumor control rate of the cyberknife in the treatment of acoustic neuroma is 85 to 100%, the hearing retention rate is 60%, and the complication rate is 5.6%.
Conclusion
Once the acoustic neuroma is diagnosed, if the tumor is large or nerves compression, and the patient has severe signs and symptoms, it should be treated as soon as possible and the goal is to protect the function of the auditory nerve and facial nerve. For elderly patients with poor health conditions, small tumors, no brainstem compression or postoperative remnants, conservative treatment can be used for regular follow-up visits and examinations, or cyberknife can be used to control the tumor growth. The specific treatment plan requires a comprehensive evaluation by an experienced neurosurgeon and the decision done by patient and patient’s family members.
Middle-aged people who suffer from tinnitus and hearing loss. Some seemingly insignificant symptoms are likely to be signs of acoustic neuroma and should be further checked as soon as possible. If the acoustic neuroma is detected and diagnosed early, the outcome will be greatly improved, and the functional retention rate of the auditory nerve and facial nerve will also be preserved.
