 Book an Appointment
Book an Appointment




2017-10-17

What should I do if the intervertebral disc herniated again?
This is a question many patients often ask after knowing that their intervertebral disc herniated again. 50-year-old Ms. Li is a housewife. In May 2016, she developed low back and leg pain after bending over to take a heavy object. After an MRI scan, it was found that the lumbar intervertebral discs of the 4th and 5th segments of the lumbar spine protruded 0.7 cm to the left (see Figure 1) indenting the left nerve root. What to do if the intervertebral disc herniated again?
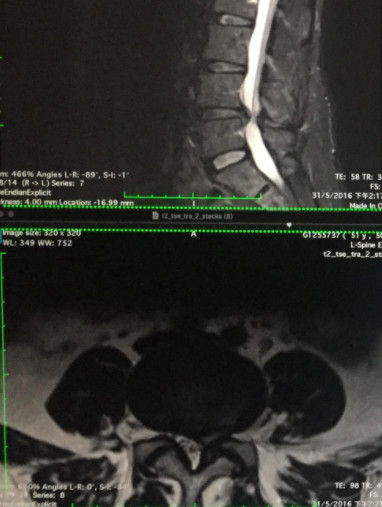
(圖一) 2016年5月腰椎第4,5節椎間盤 0.7cm向中左突出
Case Sharing
Ms. Li’s disc herniation did not improve after more than half a year of physical traction and medication. Instead, she began to feel fatigue, tension, calf cramps and numbness in her left leg, unable to travel or sit for a long time. The doctor recommends spinal nerve injection, or surgery to remove herniated disc. Ms. Li consulted the author in January 2017 and hoped to have Cox® decompression manipulation, to see if surgery can be avoided.
But because Ms. Li’s case of herniated disc has been treated with conservative physiotherapy for six months, and she has left foot weakness and frequent urination at night. She decided to perform an MRI to confirm the situation. From the MRI film taken that day, it was found that her lumbar intervertebral discs in the 4th and 5th segments had herniated by 0.9 cm, and the compression on the cauda equina was even worse than before (see Figure 2). And she has neurological deficit condition, so it is recommended that she should undergo surgery to remove the herniated disc. Ms. Li underwent minimally invasive surgery to remove herniated intervertebral discs on January 15, 2017. After the operation, her previous low back pain and leg weakness were greatly improved.
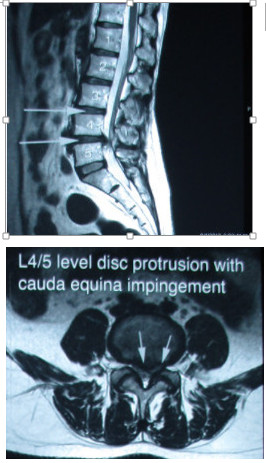
(圖二) 2017年1月腰L4/5椎間盤嚴重突出, 0.9cm壓向馬尾神經線
After the minimally invasive surgery of the herniated disc, the doctor advised that she should completely avoid lifting heavy objects, not doing exercises or bending after the operation. Unfortunately, the patient did not comply. Three weeks after the operation, Ms. Li’s lumbar disc herniated again in the 4th and 5th lumbar vertebrae (see Figure 3), so that the legs and buttocks are painful and numb. The patient did not want to have another operation in a short time, and the condition was not serious, so she accepted the Cox® decompression manipulation. After 30 times of Cox® decompression manipulation for four months, the pain and numbness of the patient’s legs and buttocks disappeared. The MRI comparison showed that the re-protruding disc after the operation was significantly reduced and reabsorbed, and the previous compression of the nerve was also improved (see Figure 4). The patient now maintains monthly Cox® decompression manipulation to maintain the disc condition.
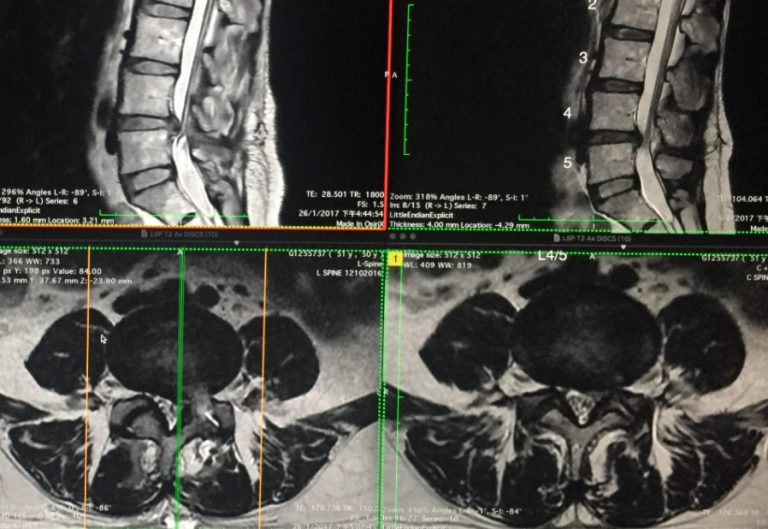
(左圖三) 術後3星期因做家務腰椎第4/5 節椎間盤再次突出 (右圖四) Cox®椎間盤脊椎神經減壓治療後, 再突出的椎間盤明顯縮小及回收, 之前壓著神經的影象也改善不少
Minimally Invasive Discectomy
Minimally invasive discectomy is a surgical operation that can reduce the pressure on the nerve roots and spinal cord caused by a herniated disc. The neurosurgeon will make a small cut in the patient’s low back and remove some or all of the intervertebral discs. In some cases, the doctor will also remove some of the vertebrae to relieve symptoms caused by compressed nerves. Traditional open spine surgery has large wounds and separates muscles. Minimally invasive surgery has only one small incision or multiple small incisions, and because of the use of muscle retractor, neurosurgeons can separate muscles around the spine without cutting muscles. This method preserves the function of muscles and blood vessels around the spine. The patient undergoes the operation under general anesthesia. The doctor first makes a small incision in the patient’s low back then puts in a dilator to gradually expand or separate the muscles and structures of the low back, and remove the intervertebral disc or bone spurs that press the nerves. The muscle and incision are sutured.

微創手術只有一個小切口
Care tips after surgery
Two to three days after discectomy, a low back brace can be worn at all times except for meals and sleep. When getting out of bed, lie on your side, lift up your body with the strength of your arms, and at the same time, hang your feet under the bed and sit up. After getting out of bed, you can stand, walk, avoid sitting or standing for a long time. When standing, keep your spine straight, hold your abdomen, and bend your knees slightly, which can reduce spine pressure. Flat shoes or sports shoes should be worn. High heels should not be worn. The shoes should have an anti-slip function. For six to seven days after the operation, you can sit on a chair with a hard surface with a back support. The sitting posture must be correct. Do not bend and twist your body, or sit on the chair twisting the body.
In the first week, short walks, driving , heavy lifting and sports are not allowed.
In the second week, you can sit, stand, walk and drive short distances for a short time, but still not exercise.
In the third or fourth week, you can do some light work, but actions that cause back pressure are absolutely prohibited, such as lifting heavy objects and twisting the lower back.
Do not sit for too long in the fourth to sixth weeks, stand and walk as much as possible.
In the eighth week, you can start doing light work, but you must still avoid twisting and lifting heavy objects.
In the twelfth week, the previous workload can be restored, but avoid heavy lifting.
Avoid overwork on the neck, upper back, and lower back for half a year to a year to prevent re-protrusion of the intervertebral disc.
Surgery procedure and post surgical care
The purpose of discectomy is mainly to relieve the symptoms of nerve compression and avoid more serious damage to the compressed nerve. Patients should consider surgery if they have the following serious symptoms:
1. Unbearable pain occurs, or the use of any medicine cannot relieve the pain in the back or legs.
2. Seriously affects daily activities or experiencing incontinence, which is called cauda equina syndrome.
3. After receiving conservative treatment for more than three to six months, the pain or numbness cannot be relieved.
4. During conservative treatment, nerve defects still occurred.
As for the post surgical treatment after discectomy, the purpose is to help patients relieve postoperative pain and leg numbness, and at the same time restore the movement function and flexibility of the spine. Cox® decompression manipulation is a safe and effective treatment method. According to medical clinical research and evidence, it has a significant effect on disc herniation or condition after discectomy. Generally, patients can receive Cox® decompression manipulation 6 to 12 weeks after the operation; if the patient has undergone spinal fusion, the treatment can be started 12 to 16 weeks after the fusion surgery; if the disc herniation is found again after the operation, they can receive the treatment immediately.
*Please refer to COX TECHNIC official website www.coxtechnic.com
